
Peter wrote:
This makes the NHS workforce vulnerable to any illness which hits a lot in one go. If it was ingrowing toenails, it would be the same problem.
Well, not really.
Even if the NHS was staffed by nothing but perfect physical specimens, with every staff member doing at least 200 minutes exercise per week, and all bang in the middle of “normal” BMI, and not a single staff member having any conditions that pose extra risk, the fact is that COVID will still have you off work for a minimum of 3-5 days with a mild case, with on top of that a minimum legally enforced self-isolation period on testing positive (meaning anyone who has to be present at work, and cannot WfH – which in the NHS is anyone who is not an actual administrator, is off work for that entire period). If there is a rapid rate of COVID infections in the NHS, it whacks it, even if not a single NHS staff member gets more than the sniffles.
Same with any occupation which requires physical presence – since you end up in quarantine on catching the thing, if a lot of people catch it at once, that business is going to struggle until people come out of quarantine. The businesses that can get away with a relatively light impact are those who are doing jobs where they can work from home, because then they are only off work for the acute period, and can continue to work in quarantine. (Anecdotally, everyone I know who is vaxxed who has caught symptomatic COVID have generally been off work sick for 3 or 4 days, and those who can WfH have been well enough afterwards to do so for the remainder of the quarantine period).
Ingrowing toenails aren’t contagious and don’t require people to quarantine.
Fair enough, but is that a reason for locking down the rest of the country?
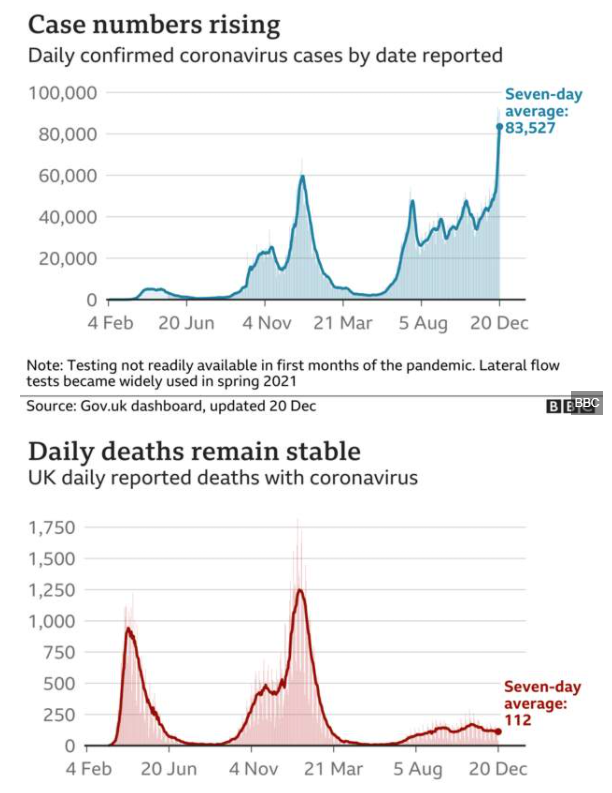
The UK data is fairly similar to SA:
For the UK, it is too early to tell.
Certainly, the general idea – we vaccinated enough, so let’s open up, even in the face of Delta – has worked.
For Omikron, we will have to wait two more weeks to see what it really does.
South African hospitalisation data is encouraging and it looks like the hospitalisation rate is lower than in the previous wave. How much that is due to vaccination, or natural immunity is not clear.

For comparison – the case numbers. Please note that the hospitalisation graph starts at week 35, where case numbers were comparatively low, it is NOT the previous peak.

This is from the South African source for consistency.
So the truth may well be somewhere in the middle – combined with vaccination it is milder than previous strains (but certainly not “harmless” / “common cold”), but the speed of the spread is cause for some concern.
alioth wrote:
Even if the NHS was staffed by nothing but perfect physical specimens, with every staff member doing at least 200 minutes exercise per week, and all bang in the middle of “normal” BMI, and not a single staff member having any conditions that pose extra risk, the fact is that COVID will still have you off work for a minimum of 3-5 days with a mild case, with on top of that a minimum legally enforced self-isolation period on testing positive (meaning anyone who has to be present at work, and cannot WfH – which in the NHS is anyone who is not an actual administrator, is off work for that entire period).
Your point holds because of the enforced self-isolation, but I don’t believe it’s true that even a mild case has you off work for 3-5 days purely because of the effect it has on you.
Over 50% of infections are asymptomatic and undetected, and many/most of the symptomatic ones are so mild that, were it not for the required self-isolation, people would not take time off work. I will adjust that assertion somewhat though, because the NHS is public sector and public sector workers generally have lower thresholds for the severity of illness necessary to be off work.
Mooney_Driver wrote:
The fairy tale that Omikron creates mostly mild cases is unproven, unfounded and outright wrong
The latest I have read (yesterday), omicron affects the lower lungs less hard than previous strands.
One of the “chief scientists” has just confirmed what’s been known for a few days (prob99 he was not authorised to say anything that wasn’t “on message”  ) – 50% of cases in the hospitals are people who got there for some other reason and were subsequently tested positive!
) – 50% of cases in the hospitals are people who got there for some other reason and were subsequently tested positive!
There is no reason to suppose it is any different elsewhere in Europe.
Maybe once people have finally come to the acceptance that the world as we knew it pre-corona HAS ended 2 years ago, we might find another base for discussion.
Let’s see what happens. However, we don’t need the repeated message of total impending doom. Even as pilots, we are trying to organise trips and meet-ups (there is one to Aosta / Cervinia in mid-January 2022) and these are very doable, to countries which have not actually shut.
For some amusement, when I was in Cervinia last week, I heard a story from one of the instructors on how one could ski in “closed” Switzerland. Due to the big publicity in Italy in Oct 2020, showing queues at the lifts, the lifts were shut after just 1 day’s opening, so there were no lifts running in Italy. The way the Italians skied was

The Italian slopes were open only for “elite athletes” or for people under training, so instructors were doing well
It was a wasted economic opportunity to chuck away the 20/21 winter, especially after the vaccine arrived, especially to people testing negative, because the way the slopes are now set up, it is really safe, and it isn’t rocket science to work out how to do it. It just took some political balls.
omicron affects the lower lungs less hard than previous strands.
Yes; it hangs around at the top end, so it travels more easily (via aerosol) but doesn’t hit the victim much – just like the common cold which also lives “up top”. This was stated today by one scientist but he had to quickly qualify it as uncertain otherwise, one assumes, his funding would be pulled.
Peter wrote:
50% of cases in the hospitals are people who got there for some other reason and were subsequently tested positive!There is no reason to suppose it is any different elsewhere in Europe.
This should come at no surprise and is the result of successful vaccination reducing Covid hospitalisation. Currently, around 2% of people in the UK have Coronavirus [defined as testing PCR-positive; the latest ONS statistic is around 1 in 60] so all things being equal, 2% of the hospital population will have a positive diagnosis. Around 5% of the hospital population is reported to have Covid (all patients are routinely tested using a PCR test), so the 2% are roughly half of that.
This is not exact, but half is about right.
If Omikron is less aggressive than Delta, this will become even more skewed.
Peter wrote:
The UK data is fairly similar to SA:
Omicron share in UK is still below 40% – and below 5% before Dec.10th. So the fact that the infections between June and November did not lead to as many deaths as in the Feb wave, can impossibly be caused by Omicron.
On the other hand between the last wave with massive fatalities in your data and the current wave with much lower fatality rate even before Omicron had arrived, the vaccination rate in the UK went up from <5% to > 65%.
It’s vaccination that helps to prevent deaths, not Omicron.
Cobalt wrote:
South African hospitalisation data is encouraging and it looks like the hospitalisation rate is lower than in the previous wave. How much that is due to vaccination, or natural immunity is not clear.
It’s interesting to see what happens in SA – but really hard to judge from one wave in one country what the impact of the virus variant really is – we will know in Feb/Mar when we have different data from different countries. One should also not forget, that summer waves in the past have been generally less lethal than winter waves.
Graham wrote:
but I don’t believe it’s true that even a mild case has you off work for 3-5 days purely because of the effect it has on you.
I know it’s just anecdote, but every person I know who have had a symptomatic case has been off work (including WfH) for 3-5 days due to the symptoms which have included fatigue and brain fog (which isn’t uncommon with viral infections, I’ve had viral infections in the past with these symptoms – you might be walking around and generally vertical, but trying to do anything that requires any thought is slow and exhausting). It’s hard to do any work which requires concentration with the typical mild symptoms. These people all of course had delta. Perhaps the omicron variant doesn’t give you ‘brain fog’.
Those “waves” are really not all that relevant. When looking at the world as a whole, it’s a constant 500k per day getting infected with a ripple superpositioned on top. Clearly the amplitude of that wave is diminishing. What’s the cause and effect of that wave? The first wave is pretty obvious. The next ones are not very obvious. It could be caused by new strands, it could be caused by changing restrictions, it could be caused by changing travelling patterns, seasonal changes affecting the virus and so on.

Also, these strands themselves are not spreading equally about. SA has had a “beta” strand that is not very evident in Europe. Omicron has completely taken over in SA. It is on full rise in the UK and Norway, but not in any other Scandinavian country, or in Germany. It’s the delta strand that is dominant.





